










COVID-19 PREVENTION AND IMMUNITY BOOSTER
Here's the outline...there's still time to launch this on a war footing before situation goes out of control like in Italy..
1. THE BEST DEFENSE FOR any flu is to strengthen our Immune System year round. And Vitamin D3 does precisely that! Luckily in India, D3 (Cholecalciferol) “Arachitol” injections in 7.5mg (300,000 IU) and 15mg (600,000 IU) are available on prescription at most hospitals in India and doses of 100,000–300,000 IU have been administered intramuscularly 6-monthly or once-yearly quite safely.
A single therapeutic annual intramuscular injection of 600,000 IU (15mg) cholecalciferol is currently being used to treat vitamin D deficiency in India and Canada, and its safety has previously been evaluated. Read this linked Research on "Annual intramuscular injection of a megadose of cholecalciferol for treatment of vitamin D deficiency: efficacy and safety data".
https://www.ncbi.nlm.nih.gov/pubmed/15992330/
In the US, D3 60000 iu Caps from Biotech Pharmacal is good. Dr. John Jacob Cannell MD of Vitamin D Council, USA states "As I weigh 220 pounds (100 kg), I would take 200,000 IU per day for seven days if I thought I had an infection with a 1918-like influenza virus."
In India, that's 1,400,000 IU or about equivalent of two Injections of Arachitol 15mg (600,000IU). And I believe each injection costs a measly Rs.30/- ! Everyone can easily afford it!
2. Here's a presentation from Dr. Seheult, MD 'Vitamin D may aid in prevention of COVID-19": watch from 2:04...
3. Outline of the Campaign:
What?
"COVID-19 Prevention and Immunity booster" Community Campaign
Where?
Any gated community for starters or a designated area/ territory.
When?
Immediate on a war footing.
How?
Campaign strategy
1. Collect/gather updated Demographic count for all households within the community
Elders 60+
Adults 21 to 60
Children/Teen upto 21
(this data should be available with the community administration)
Conduct Vitamin D3 lab tests thru tie-up with Thyrocare, LabCorp and similar...to segregate vitamin D deficiency cases.
2. Procurement:
For India:-
a. Arachitol 3L/6L injections from Abbott and
b. Calcigen D3 1x4 softgel capsules from Cadila in bulk, quantity based on demographic data.
As this is for a social cause, their CSR initiative may deliver free.
For USA :-
D3 60000 iu Caps from Biotech Pharmacal
3. Assign lead Doctor and several nurses for the Campaign. Announcement to residents of staggered dates of administrating Arachitol block wise.
4. Arachitol 3L/6L injection administration Through Mobile Ambulances, Nurses can administer intramuscular.
5. Distribution: of Calcigen D3 60kiu softgel capsules; pack of 5 per family.
Residents can take a D3 lab reTest after 8 weeks..
Close monitoring of the gated community for any further spread of the Sars-Cov-2 virus or if its being contained within.
______
Some research papers for the Doctors review..
1: Vitamin D for Prevention of respiratory tract infections...
2: Vitamin D and the Immune system.. https://www.ncbi.nlm.
3: Forget C, D may be the vitamin for cold and flu protection. Study...
4. COVID-19 Coronavirus can most likely be fought by Vitamin D...
Suggested Injection and Capsules:
Arachitol, Arachitol Nano
Mfr: Abbott India
Calcigen D3 Softgel by Cadila
4. Living Example on Toxicity :
In the US, Author's 25(OH)D test at LabCorp USA resulted in a dangerously low 12.2 ng/ml. Over the following 8 weeks, he inadvertently consumed a total 2,260,000 IU over 56 days averaging daily to about 40,000 IU ! His subsequent LabCorp test result was 239 ng/ml ! Its very high when one considers the normal range between 32-100 ng/ml and some may even call this beyond toxic!! Truth is, he never felt any better!
His humble role in this is simply to provide comfort of confidence both to the medical fraternity and the citizens as a Living example of a person who has consumed very high levels with no side effects or toxicity and he has LabCorp USA test results to back it up.
LabCorp, USA, is a leading global life sciences company that is deeply integrated in guiding patient care through its comprehensive clinical laboratory and end-to-end drug development services.
5. On Toxicity : Mayo Clinic Research:- Vitamin D toxicity is rare in people taking supplements..
Above rounded research data validation should satisfy the Medical fraternity advising the Govt for implementation of the campaign in densely affected areas. If administering Arachitol injection intramuscular is an issue, providing higher dosage of D3 capsules supplements will also help.
Meanwhile, due to the emergent nature of the situation and the probability of exponential escalation, it would be helpful to the society at large, if you can initiate a "COVID-19 Immunity Boister" mailer to your Twitter/FB groups participants with this post link. This will also be a timely initiative!
Stay safe, stress free and warm. God bless all.
Stay safe, stress free and warm. God bless all.
UPDATE: MagicPlan Retire & Enjoy
Here's the updated Spreadsheet that is more cleaner and easier to understand. Thanks to Ashal Jauhari's feedback on Bonus Rates differential:
 There's been an overwhelming response to the previous post clearly validating that many have been impacted. An excel template is under preparation and will be posted shortly.
There's been an overwhelming response to the previous post clearly validating that many have been impacted. An excel template is under preparation and will be posted shortly.
#Life Insurance #MagicPlan

#Life Insurance #MagicPlan
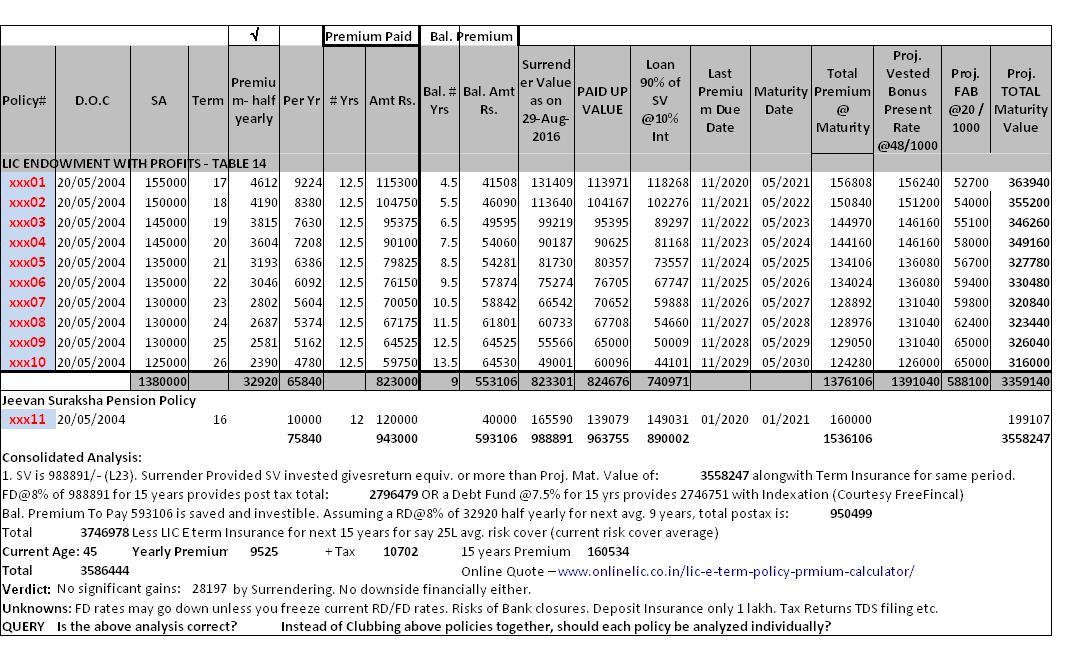
LIC policies Magic Plan – Retire & Enjoy! Surrender or Continue?
LIC policies Magic Plan – Retire &
Enjoy! Surrender or Continue?
Here's a case of an IT Engineer lady who
was 'sold' a total of 11 policies per above plan:
Date of Commencement of all eleven
policies was May 2004 with each policy maturing in 17,18,19, 20, 21,
22, 23, 24, 25, 26 years i.e first one matures when she turns 50 and
last one matures when she turns 60.
In terms of premiums, she pays a
total of 65840/- per year and has already paid for 12.5 years (2nd
half yearly premium of 32920/- is due in November 2016). So for the
first policy with SA of 155000 she has 5 years left to pay premiums,
2nd one 6 years, 3rd one 7 years and so on until 10th
14 years. She says the LIC agent introduced to her through a good
friend, had a look at her pay slip (she was naive) and
proposed her immediate savings under Sec.80C plus of course Retire &
Enjoy! She was told that from year 2021 onward, she doesn't have to
pay any more premiums but enjoy annual maturity values between Rs.2.5-3
lakhs for the next 10 years with Risk Cover (operative word should
have been the premiums for rest of the policies are deducted from the
maturity value of earlier year policy). Additionally, the 11th
policy was Jeevan Raksha Pension Policy with annual premium of
Rs.10000/- for 16 years.
Although it seems a bit late in the day
to consider surrendering above policies after having paid premiums
for 12 years, I could see that for half of these policies, she still
has to pay premiums for 10+ years. So I decided to dive deep and
analyze an answer to the following questions:
- Will it be financially productive to surrender the policies now?
- Upon surrender, will the SV enable the policy holder to recoup her 'losses' so to speak?
- Will alternative safe investments provide her returns over & above the Projected Maturity value?
First task for her was to get the
Status Report and Surrernder Value Quotation from LIC which she did. Based on the data in these reports, I
set out to enter the values in a Spreadsheet which is easy for any
layman to understand. I also tried to unravel the calculations using
a Surrender Or Paid up calculator. Below is a snapshot of the
Spreadsheet:
NOTES:
Above sheet is a consolidated analysis
to provide broad picture for better decision making. Perhaps results
may slightly vary if each policy is analyzed individually. Key
takeaway: the policy holder has lost previous 12 years of investment
returns or about 30 lakhs. If she had NOT been sold this policy, then
her premiums invested would have given her approx. 65 lakhs by the
last policy maturity due date in 2030. But then, its like saying had
one invested in Wipro in 1980, I would have been a crorepati today!
Going forward from here, there's
negligible difference between the maturity amount from LIC and the
returns from risk free RDs/FDs. So the verdict might as well be to
reconcile and continue to pay the balance premiums.
Is there any angle not covered in the
above? Inflation? Are there any other options not considered? No
Equity based investment considered due to risk factor plus
comparison had to be apples to apples.
Your views are welcome.
Above chart has been updated....
http://vishigan.blogspot.com/2016/08/update-magicplan-retire-enjoy.html
Above chart has been updated....
http://vishigan.blogspot.com/2016/08/update-magicplan-retire-enjoy.html
The Antioxidant Paradox & the Goldilocks Principle | Stock Gumshoe
"Just Right" Common Sense on
Salt, Antioxidants, Blood Pressure and Obesity

LINK
Microblog: The Antioxidant Paradox & the Goldilocks Principle | Stock Gumshoe
Posted on
[ed. note: We've been privileged to share with you some "non investment" commentary here from Michael Jorrin, a longtime medical writer who we like to call "Doc Gumshoe" -- today he's got a new piece for us that should help us think skeptically about yet more of the "easy solution" promises people make about health, usually when they're trying to sell you the latest hot supplement or drug ... and, as always, we need to remind you that the opinions from Doc Gumshoe are his own, we've done no more than a bit of light editing to prepare his piece for you today. Enjoy!]
That’s the Received Wisdom, and I won’t argue with it, because there’s certainly an element of truth there. How large or important that element of truth is remains to be seen. Let’s take this catechism one bit at a time.
Free Radicals: What Are They, Anyway?
First, what are free radicals? They are not bomb-throwers who have evaded prison, but small ionized chemical entities that are avid to combine with whatever they can latch on to. Consider saltpeter, chemical name potassium nitrate, chemical formula KNO3… Saltpeter is used as a food preservative, particularly in cured meats, and supposedly was put into the food of boys in boarding school, soldiers, and other young libidinous males in order to curb their natural instincts. When potassium nitrate enters solution, such as the human bloodstream, it immediately ionizes, meaning that the potassium part and the nitrate part swim around independently. The potassium ion has an extra electron in its outer shell, so it is K+, and the nitrate part is missing that outer electron, so it is NO3 –. The NO3 – ion is a free radical, and it seeks to combine with other entities from which it can grab that missing electron.

Saltpeter is just a single example of the kinds of substances that we’re exposed to that can create free radicals. All kinds of substances can lead to free radical formation – anything that can release ionized oxygen, hydroxyl, hydrogen peroxide, or other oxidizing ions. The worst offender is cigarette smoke, and there are many more in our environment. In the process of swiping electrons, free radicals can affect and perhaps damage human cells, including their DNA. If the damaged cells merely perish, that’s no big deal – cells die all the time and are replaced by new, healthy cells. But if cellular DNA is damaged, the successor cells themselves may be damaged or even cancerous. That’s the chief threat posed by free radicals.
What Do These Wonderful Antioxidants Really Do?
Antioxidants counteract the effects of free radicals by offering themselves up as targets, sparing some of the human cells that the free radicals might otherwise have damaged. There are lots of antioxidants in the food we eat, not just pomegranates and blueberries and cherries and carrots. The question is, are these dietary antioxidants sufficient?
There are those who answer that question with a resounding “NO!!!” (Many of these folks are the makers and marketers of antioxidant supplements, so they may not be totally disinterested.) Whether this view is completely fact-based or not, it plays nicely into a common tendency, which is that if a bit of something is good for you, then more of that same something is probably even better for you. Advocates of antioxidant supplements point out that, while antioxidants in our food may have been sufficient in times past, we’re exposed to so many more free radicals than our ancestors were that we need supplemental antioxidants.
In the case of antioxidants, this is open to question, at the very least.
So, what are antioxidants? The antioxidant substances in those useful (and pretty good-tasting!) foods are flavonoids, carotenoids, polyphenols, and others. Carotenoids, especially beta-carotene, are precursors of vitamin A, and vitamins C, and E are themselves antioxidants.
Dietary Antioxidants vs Antioxidant Supplements
The evidence that dietary antioxidants help prevent disease is quite strong. For example, there was a large study in Sweden, which followed more than 30,000 women for more than 11 years. The total study population was divided into fifths, and the study found than the women who consumed the most antioxidants in their diet (the top fifth) had an incidence of heart failure that was about 60% of that in women who consumed the least antioxidants (the bottom fifth). Heart failure is a pretty good indicator of many health factors, since several factors contribute to heart failure – high blood pressure, elevated cholesterol, diabetes, and obesity.
However, when it comes to antioxidant supplements, quite a lot of the evidence points the other way. For example, a study in current smokers who were given beta-carotene supplements found that these appeared to increase rather than lower the incidence of lung cancer.
The vitamin E question is particularly complex. The antioxidant found in vitamin E supplements is alpha-tocopherol, while the vitamin E antioxidant found in food is gamma-tocopherol. Vitamin E in the diet may reduce the risk of heart disease and cancer. Not so with vitamin E supplements, perhaps because of the difference between the alpha- and gamma-tocopherol.
In fact, rather than being beneficial, antioxidant supplements may increase rather than decrease mortality.
The most convincing evidence comes from the Cochrane Collaboration, which is an international organization (28,000 contributors from 100 countries) that reviews clinical trial data from all over the world and scrupulously creates analyses that pool the data from multiple trials. Cochrane reviews are generally regarded as the gold standard.
Cochrane conducted a systematic review of studies evaluating the benefits of antioxidant supplements, including beta-carotene, vitamins A, C, E, and selenium. They reviewed 78 studies with 296,707 participants, and found that overall, antioxidant supplements significantly increased the risk of death. In the 56 trials that they evaluated as having the lowest risk of bias, antioxidant supplements increased the risk of death by about 4%. That may not sound like a huge increase in the risk, but when we consider that antioxidants are supposed to prevent disease and death, and the data tell us that that they do the contrary, that should give us pause. And, by the way, this was true for each of the individual antioxidant supplements included in the study.
Why This Apparent Contradiction?
What might account for this paradox? One possible mechanism is that, while it’s accepted that free radicals might trigger the mutations that initiate the growth of cancer, there is some evidence that free radicals also preferentially attack cancer cells rather than non-cancerous cells. So perhaps in a healthy person, reasonable amounts of antioxidants in the diet might reduce the number of newly mutated cancer cells. However, once cancer cells are present, (as in the study in smokers mentioned earlier), free-radicals might keep cancer growth in check, and antioxidants might stymie their mission.
So the question looms: what’s the right balance between free radicals and antioxidants? This is the Goldilocks Question: how much is Just Right? With regard to the free radicals versus antioxidants question, it seems to me that the Just Right option is plenty of dietary antioxidants, but go easy on the supplements.
It does appear that free radicals serve some essential function, and we don’t want to eliminate them from our bodies – nor can we, since some free radicals are actually created in our white blood cells (neutrophils and macrophages) and help to kill and scavenge bacteria, protecting us from some infections.
The Goldilocks Principle and the Search for Just Right
However, the Goldilocks Question applies to almost everything in our lives. Everybody, and I really mean everybody, knows from experience that we lowly humans are comfortable only in fairly narrow range of conditions. For example, our normal body temperature is 98.6° F (37.6° C). But if we climb into a bathtub that’s at 105° F, it feels really, really hot. And if it goes much below 95° F, we might run a bit more hot water to get it to feel just right, so that Goldilocks would be happy in the tub.
The same question can be asked of many other things – such as the Just Right amount of salt in our diets, our optimum weight range, how much alcohol should we consume, and on and on.
The Salt Question
The salt question has resurfaced fairly recently. For quite a long time, the doctrine of the health authorities (such as the U. S. Centers for Disease Control and Prevention) was that most people should consume not more than 2,300 milligrams of salt per day, and that people at risk for heart disease should limit their salt consumption to not more than 1,500 milligrams per day. That’s not much salt – maybe a bit more than half a teaspoonful.
The reason for this edict is that salt (or, actually, sodium ions) tends to raise blood pressure, and high blood pressure, as we all know, leads to heart disease, diabetes, and strokes.
But the CDC has changed its tune, based on research that has emerged since their recommendations, which they issued back in 2005. A committee convened by the CDC reviewed the current evidence and pronounced that there is no reason for anyone at all to try to limit their salt consumption to less than 2,300 milligrams per day, and pointed out that when salt consumption is pushed below that level, not only is there no benefit, but some people may begin to experience actual adverse consequences.
A common assumption is that if too much of something is bad for you, then the best thing is to have as little as possible. This is the reverse of the assumption that has been made about antioxidants, that if some is good, more is better. But the Goldilocks Principle holds that we have to look for the amount that is Just Right.
In the case of salt, we can point to a couple of studies. In one, conducted in Italy, two groups of patients with congestive heart failure were assigned to diets with different quantities of salt. One group consumed 2,760 milligrams per day, and the other consumed 1,840 milligrams per day. The patients that consumed the smaller amounts of salt in their diet had three times the number of hospital admissions and twice as many deaths as those that consumed the higher amounts of salt.
Another larger study followed nearly 30,000 patients with hypertension for nearly 5 years and tracked their salt consumption by analyzing urine samples. In that study, the risk of clinically important cardiac events, including deaths, was significantly higher at the two ends of the scale – patients consuming more than 7,000 mg per day and those consuming less than 3,000 per day. So, based on those data, the Just Right amount of salt is somewhere in between those two numbers.
I should mention here that the average sodium consumption in the US, and elsewhere for that matter, is about 3,400 milligrams per day. Is that too high? The American Heart Association still thinks so, in spite of the new CDC recommendations. A concern is that what lots of people will take from the new data is that salt just doesn’t matter, and they can use as much as they want. But that, too, is a violation of the Goldilocks Principle – what we’re looking for is the Just Right amount of salt.
(By the way, I might add here that the biggest users of salt in the American diet are not cooks in the home kitchen nor yet people who sprinkle it on at the dinner table, but salty packaged food products.)
None of this research denies the well-established link between excessive salt consumption and hypertension. What it points to is that low sodium levels have some clear harmful consequences – triglyceride levels rise and insulin resistance increases, with potential adverse cardiac consequences. We can’t judge salt consumption just on the basis of its effect on blood pressure
Speaking of blood pressure, the Goldilocks Principle applies there as well. Blood pressure is carefully adjusted by many homeostatic responses so that mean arterial pressure is about 100 mm Hg. Mean arterial pressure is just what it sounds like – halfway between the pressure at the moment when the heart contracts to force blood into the arteries and when it relaxes to accept more blood from the veins. That pressure, 100 mm Hg, is about 13% higher than atmospheric pressure at sea level, which is 760 mm Hg. We need that relatively small degree of additional pressure to keep the blood circulating throughout the body.
However, supposing your blood pressure was only 10% higher than atmospheric pressure, say, a mean arterial pressure of about 75 mm Hg, which might translate to 100/50 mm Hg. That 50 mm Hg value for your diastolic blood pressure is a shade too low. You’re running a risk of keeling over in a faint, because your heart can’t pump blood into your brain.
Of course, as soon as you do keel over, your heart isn’t pumping blood against gravity so much, and you’ll come to pretty quickly, and if you didn’t come down too hard, you’re probably fine. But that tells you that the little 3% difference between just right and too low can be important.
How About Weight and Body Mass Index?
Wasn‘t it Wallis Simpson, the Duchess of Windsor, who said “You can’t be too rich or too thin?” I don’t know about too rich – I’ll let you know if I ever get there – but you can definitely be too thin. The term for being excessively thin is cachexia; a condition that is seen in such diseases as cancer and AIDS, but that may also occur in persons who are obsessed with losing weight, e.g., some fashion models. It’s a risky condition, and can be fatal.
Of course, at the other end of the spectrum, we all know about the risks of being too fat. But is there a Goldilocks Principle here, and what does it point to as a Just Right body mass index (BMI)? Well, there’s a range, of course, but some data points to a Just Right range that’s considerably higher than the Received Wisdom.
In case you’ve forgotten, the official BMI ranges are: below 18.5, underweight; 18.4 – 24.9, normal; 25.0 – 29.9, overweight; over 30.0, obese. Taking yours truly as an example, I am 6’ 3” and I weigh about 217 pounds, so my BMI is 27.1 – in the middle of the overweight category. If I weighed 180 pounds, my BMI would be 22.5 – normal. To be underweight, I would have to weigh about 140 pounds. I haven’t been that skinny since I was a sophomore in high school, and I was really, really skinny then.
However, there’s pretty convincing evidence that those BMI ranges are flat wrong. An analysis of 40 studies looked at BMI and calculated the risk for both overall mortality and cardiovascular mortality, compared with normal weight subjects, which for this study was defined as BMI 20 – 24.9. No surprise – very obese individuals, those with a BMI over 35, were at very high mortality risk – about 10% higher total mortality, and 88% higher cardiovascular mortality. But persons with BMI values below 20 were also at very high mortality risk – 37% higher total mortality (higher than the very obese!) and 45% higher cardiovascular mortality.
What about the overweight and the obese? The merely overweight were at the lowest risk for both total (13% lower) and cardiovascular mortality (12% lower). And the obese in the 30 – 34.9 BMI range were essentially at the same risk as the normal weight subjects.
So, based on that study, which, by the way, came out of the Mayo Clinic, and included data on more than a quarter of a million subjects, the healthiest weight range is what the BMI classifies as “overweight.” The authors of the study suggested that it might be time to scrap the BMI as a risk factor. Applying the Goldilocks Principle, a bit overweight might be Just Right.
Is There a Just Right Level for Cholesterol, or Is Lower Always Better?
As far as I know, no one yet has determined what the Just Right number is for cholesterol, in particular LDL-cholesterol.
First, a word about nomenclature: we hear all the time about the good cholesterol and the bad cholesterol. I fear that those terms are just the way some health professionals try to avoid confusing us, but I think those terms are themselves confusing. I need to make the point that there is only one cholesterol, a fairly simple substance that has the characteristic of being solid at body temperature, and therefore, cannot by itself be transported in the bloodstream.
So, in order to get where it needs to go, which is just about everywhere in our bodies, cholesterol is gathered up in little bundles called lipoproteins. Some of the lipoprotein cholesterol bundles are large and loose – these are the low density lipoprotein cholesterol bundles, or LDL-cholesterol, or sometimes just LDL for short. Some are smaller, neater, tighter bundles – high density lipoprotein cholesterol, or HDL-C for short. The LDL bundles are the ones that tend to deposit cholesterol in our arteries, causing no end of trouble, therefore bad cholesterol, while the smaller HDL bundles transport cholesterol back to the liver and to the bile ducts for excretion, therefore good cholesterol.
We know what too high LDL-cholesterol levels are: in an otherwise healthy person, a reading of 190 milligrams per deciliter is way too high, placing that person at risk for heart disease. In persons with LDL-C levels greater than 190 mg/dL, treatment with a cholesterol-lowering drug, generally a statin, is recommended. Depending on risk factors, LDL-C levels as low as 100 mg/dL can trigger drug treatment, and in patients with established coronary heart disease or the equivalent, an LDL-C goal below 70 mg/dL is recommended.
So far, as regards cholesterol (whether total cholesterol or LDL-cholesterol) what has not yet been determined is How Low Is Too Low. Common sense (as well as current understanding of the role of cholesterol in our physiology) tells us that there has to be a Too Low level. After all, cholesterol is present in most of our tissues and is an essential component of most hormones; we synthesize most of the cholesterol in our system (only about 20% at most of our cholesterol enters our bodies as cholesterol), so clearly we need it. We just don’t know what the Just Right amount is.
A New Cholesterol-Lowering Breakthrough? We’ll See.
However, current drug development, being pursued pedal to the metal by at least four pharma outfits (Amgen, Pfizer, Regeneron, and Sanofi) may lead to a better understanding of the Just Right level for LDL-cholesterol.
It has been known for quite some time that some individuals have surprisingly low LDL-C levels – some young people are going around with LDL-C levels of 50 mg/dL or even a bit lower. These low LDL-C levels are likely due to a combination of genetics and life-style factors, and we don’t know much about the total health status of these individuals, other than that they’re in good health at the time. Have there been studies to follow these folks for another 25 or 50 years? I fear not – why would there be? We don’t go out of our way to look for trouble.
Just recently, though, a couple of individuals have been identified whose LDL-C levels are incredibly low – about 15 mg/dL. Their low LDL-C appears to be due to an almost freakishly unlikely genetic factor. These persons inherited mutated versions of a gene, designated PCSK9, from both parents. The PCSK9 gene, when working normally, is part of the physiologic process that unpacks LDL-C bundles and repacks the extra cholesterol they contain into HDL-C bundles for eventual excretion. When the PCSK9 gene is defective, some people develop excessively high LDL-C levels, and, as a consequence, are at high risk for cardiovascular disease.
But the mutations that these individuals with the really low LDL-C levels, rather than making these genes defective, had apparently made the PCSK9 genes super-effective. So pharma immediately saw a colossal opportunity, and launched research projects to develop drugs that would mimic the effect of these mutated genes. The drugs they have come up with are biologic drugs, which is to say, not simple chemical molecules, but complex drugs called monoclonal antibodies that attempt to duplicate the action of human agents produced by the immune system. Amgen has completed at least one Phase II trial in about 400 subjects, and their drug, designated AMG145 has demonstrated success in lowering LDL-C to 50 mg/dL in some subjects enrolled in the trials.
That would be enough for any pharma to mount a really big fireworks display, since no current drug or drug combination has achieved anything comparable. A person with high LDL-C, say 160 mg/dL, might bring it down to something in the neighborhood of 100 mg/dL by using a high dose of a statin. So a drug that would reduce LDL-C to half that level would be a huge step forward – in controlling LDL-C, at least!
Why do I stick in that slightly negative comment? Because we do not know the long-term consequences of living with an LDL-C level that low. The studies so far have not looked at clinical benefit – only at the change in blood LDL-C levels. Now, to be fair, the experience with lowering LDL-C has been, up to now, that heart disease risk goes down at the same time, so it would be expected that the same relationship between lowering LDL-C and heart risk would continue to hold.
But until this is confirmed by clinical trials with actual, concrete health benefits as outcome measures, we won’t know. I say this because of the Goldilocks Principle, which seems to apply in all kinds of areas where we human beings interact with the world around us. We saw what happens with antioxidants, salt, and our body mass index. We can’t assume that because some antioxidants in our diet are a good thing, more and more antioxidants are better. We can’t assume that because too much salt in our diets is bad, we should reduce our salt intake to almost nothing. We can’t assume that you can’t be too thin (I don’t know about too rich!) Similarly, we can’t assume that there are no health consequences to lowering LDL-cholesterol to previously almost unheard of levels. We’ll have to wait until we see whether those new drugs really do decrease heart disease, and whether there’s a minimum LDL-C level below which people might develop hitherto unsuspected problems.
Goldilocks is still waiting for Just Right!
* * * * * * *
Doc Gumshoe looks forward to your comments, and, in particular, to any hints about topics that you’d like to hear more about. Remember that I am not a bona fide MD, but I do keep up with health news and medical literature and consider it from my naturally contrarian point of view. My best to all, Michael Jorrin
India's FDI retail saga: From Wal-Mart to Agarwal-Mart?
 |
| By opening up retail, Indians may end up consuming cheap, low grade, mass-produced, industrial quality produce like Americans. So which way do we go? |

LINK
India's FDI retail saga: From Wal-Mart to Agarwal-Mart?

By opening up retail, Indians may end up consuming cheap, low grade, mass-produced, industrial quality produce like Americans. So which way do we go?
WASHINGTON: "I actually did vote for the $ 87 billion (war funding) before I voted against it," was a line that destroyed John Kerry's presidential campaign in 2004. He could never live down the flip-flopper reputation after opponents simplified his statement to "I was for the Iraq War before I was against it." Subtle nuances and elegant explanations, not to speak of a possible change of heart after things went south, were lost in the verbal melee in an atmosphere where you were either "for it or against it."
Something similar is happening in the debate in India about foreign direct investment in the retail sector, in which the American superstore Wal-Mart has become the figurehead. You are either for FDI or against FDI; Wal-Mart is all good or pure evil. Look, look ... says one distinguished opposition leader now in his twilight years, even Americans (or New Yorkers) are against it. Of course, some Americans are against Wal-Mart; many are for it. Many Americans are also pro-outsourcing. And anti-globalization. And pro-China. And, anti-China. It's never black and white.
In fact, as the popular Facebook-era metaphor goes: It's complicated. As someone who divides his time between US and India, here's my $0.02, or Rs 1.06 at the current exchange rate, about the FDI/WalMart debate: I am against Wal-Mart in America, and for Wal-Mart in India. How's that for a $2 Made-in-India flip-flop — or "double standard" as a colleague put it? I am also mostly vegetarian in the US, but have no problems eating non-vegetarian in India. And there's a connection between the two.
The simple explanation for all this is the US and India are at different stages of market economics, especially in the in production, distribution and marketing of food produce. The US has made some awful mistakes in embracing its current food cycle, the same way it has erred espousing a mindless automobile revolution. So while adopting the "good" that FDI retail/Wal-Mart can offer, there is no compelling reason for India to follow the US model to the T; it need not make the same mistakes. Call it retail revolution with Indian characteristics, if that is possible.
Let's break it down with examples by first looking at the "good" that the proposed retail revolution can bring into India, some of which has been articulated by ardent votaries of FDI. First off, it will improve supply chain logistics, including cold storage, and broadly bring India further in tune with 21st century western style market economy. It will save the 30 per cent wastage of perishables that we have been moaning about for 30 years. Of course there is always the question about whether it is better to eat fresh produce never mind the wastage, or whether to can the waste and eat preserved food. We'll come to that later — the simple answer could be it is better to eat something than nothing at all ...
Initially at least, the so-called FDI revolution in retail will provide better prices and returns to farmers through better yields, productivity, and distribution. It could also offer more choice, better quality, greater uniformity, improved display and packaging. All this is not a given and will not necessarily improve your health or quality of life. In fact, it could be the other way around. Here's how it has panned out in America.
The corporatization of the food chain has its upside — and downside. Farmers are coaxed — or forced — to improve yields, attain the kind of quality and uniformity that corporate interests demand, and as a result may get more remunerative prices, at least in the beginning. But it also edges out the small and marginal farmer, vastly reduce farm labor (with increased mechanization), and result in mediocre but commercially viable produce. In fact, this prospect brings home the very malaise that more "advanced" western societies are starting to realize and wanting to avoid or reverse. This is where you want to continue buying from the neighbourhood push-card vendor in India who's bringing in fresh produce to your doorstep from a local grower rather than the retail chain with its stock of mass produce whose provenance and vintage is unknown. This is where more and more westerners, at least those who can afford it, are switching to shopping at farmers market with local produce even though it is much more expensive than supermarkets.
So why is it produce cheaper (or will eventually become cheaper) in the supermarkets, you ask? Because, the economies of scale make big chain produce much cheaper. They also have deeper pockets to suffer initial losses and eliminate competition, as Wal-Mart has demonstrated in many countries.
What modern retail in the west has done is introduced food produce not just on an industrial scale but on an industrial quality too. And this is where my "prefer vegetarian in US but okay with non-veg in India" choice kicks in. That massive ten-pound pack of chicken breast at dirt cheap price ... we really have no idea of its origins or vintage. Wait ... we do have a rough idea. It was raised in a massive chicken farm owned by a corporate monopoly in methods and circumstances that will make you puke. Chicken (or cattle) that are cooped up in the dark, medicated, and force-fed continuously so that they attain maximum weight in the minimum time with minimum movement and metabolism. That's how corporates maximize profit. In India, you still have to the option of seeking out the healthier free-range or home-grown chicken, fresh locally grown- or sourced vegetables and fruits. You could be saying goodbye to all that (or at least end up paying much much more) with the FDI fiesta.
On a recent trip to the great American outback, your correspondent saw visual evidence of what this corporatization and industrialization of food production — widely seen as inevitable once the retail FDI gates are open — can do to the landscape and population. Thousands upon thousands of acres of farmland, typically owned or leased by corporates or large farming interests, grew bounteous harvests of corn (even in a drought year). This was not the corn, the "bhutta" from the push cart vendor that you eat with relish. It is mostly genetically modified, tasteless, industrial-grade rubbish that is aimed at maximizing yield. When it is not used as animal feed, it is turned into corn syrup which is used sweeten almost everything you see in the supermarket, including that sugary soft drinks you guzzle.
The result is all too visible in much of the US, nowhere more than the heartland of the country, where people come in large, economy size, with consequent health issues (obesity linked diabetes and heart disease). Much of this comes from eating cheap, low-quality, industrial grade food — from mass-produced breads and meat. There are few places in the world is where food available as cheaply (relative to income) as America. Till a couple of decades ago, Americans spent up to 15 per cent of their income on food; it is now below ten per cent and still dropping. It is now an accepted fact that the poorer the state in America, the more obese people are, because they are eating cheap, mass-produced food of the kind offered by fast-food chains. That dreadful burger and pizza and cola that you are wolfing down from the retail assembly line ... it's the cheapest and the worst kind of food you could be eating.
So here's the equation. If you allow the kind of retail revolution that has overtaken America, you could end up consuming cheap, low grade, mass-produced, industrial quality produce. Of course, it is easy to sniff down at all this from the high vantage point of those who have money in the pocket and the luxury of choice. But what about those with limited means who cannot afford to spend as much on fresh produce as corporatization of the food chain takes hold? So should be just reject the American/western way and stick to our current way, as many of those opposed to the Wal-Mart way are recommending? Then what happens to the farmers who seek better market access and greater returns, who want to eliminate waste and spoilage. Isn't FDI retail lucrative for him — at least to begin with, before predatory practices set in. Which way should we go? Will we, to paraphrase John Kerry, end up being "for it, before we turn against it?"
The answer, without it sounding like a cop-out, is to embrace the middle way. We need all the systems and logistics that FDI retail will bring, but we need to tweak it to make sure we don't go the American way. In some ways we should be reassured by what has happened already: the arrival of American retail food chains such as KFC, McDonalds, and Pizza Hut, did not destroy Indian eateries or Indian eating habits. We took the best practices from them, and today many Indian food outlets have the same look and feel of their western counterparts while continuing to serve the Indian palate. So the arrival of Wal-Mart may just herald the birth of the Agarwal-Mart.
Something similar is happening in the debate in India about foreign direct investment in the retail sector, in which the American superstore Wal-Mart has become the figurehead. You are either for FDI or against FDI; Wal-Mart is all good or pure evil. Look, look ... says one distinguished opposition leader now in his twilight years, even Americans (or New Yorkers) are against it. Of course, some Americans are against Wal-Mart; many are for it. Many Americans are also pro-outsourcing. And anti-globalization. And pro-China. And, anti-China. It's never black and white.
In fact, as the popular Facebook-era metaphor goes: It's complicated. As someone who divides his time between US and India, here's my $0.02, or Rs 1.06 at the current exchange rate, about the FDI/WalMart debate: I am against Wal-Mart in America, and for Wal-Mart in India. How's that for a $2 Made-in-India flip-flop — or "double standard" as a colleague put it? I am also mostly vegetarian in the US, but have no problems eating non-vegetarian in India. And there's a connection between the two.
The simple explanation for all this is the US and India are at different stages of market economics, especially in the in production, distribution and marketing of food produce. The US has made some awful mistakes in embracing its current food cycle, the same way it has erred espousing a mindless automobile revolution. So while adopting the "good" that FDI retail/Wal-Mart can offer, there is no compelling reason for India to follow the US model to the T; it need not make the same mistakes. Call it retail revolution with Indian characteristics, if that is possible.
Let's break it down with examples by first looking at the "good" that the proposed retail revolution can bring into India, some of which has been articulated by ardent votaries of FDI. First off, it will improve supply chain logistics, including cold storage, and broadly bring India further in tune with 21st century western style market economy. It will save the 30 per cent wastage of perishables that we have been moaning about for 30 years. Of course there is always the question about whether it is better to eat fresh produce never mind the wastage, or whether to can the waste and eat preserved food. We'll come to that later — the simple answer could be it is better to eat something than nothing at all ...
Initially at least, the so-called FDI revolution in retail will provide better prices and returns to farmers through better yields, productivity, and distribution. It could also offer more choice, better quality, greater uniformity, improved display and packaging. All this is not a given and will not necessarily improve your health or quality of life. In fact, it could be the other way around. Here's how it has panned out in America.
The corporatization of the food chain has its upside — and downside. Farmers are coaxed — or forced — to improve yields, attain the kind of quality and uniformity that corporate interests demand, and as a result may get more remunerative prices, at least in the beginning. But it also edges out the small and marginal farmer, vastly reduce farm labor (with increased mechanization), and result in mediocre but commercially viable produce. In fact, this prospect brings home the very malaise that more "advanced" western societies are starting to realize and wanting to avoid or reverse. This is where you want to continue buying from the neighbourhood push-card vendor in India who's bringing in fresh produce to your doorstep from a local grower rather than the retail chain with its stock of mass produce whose provenance and vintage is unknown. This is where more and more westerners, at least those who can afford it, are switching to shopping at farmers market with local produce even though it is much more expensive than supermarkets.
So why is it produce cheaper (or will eventually become cheaper) in the supermarkets, you ask? Because, the economies of scale make big chain produce much cheaper. They also have deeper pockets to suffer initial losses and eliminate competition, as Wal-Mart has demonstrated in many countries.
What modern retail in the west has done is introduced food produce not just on an industrial scale but on an industrial quality too. And this is where my "prefer vegetarian in US but okay with non-veg in India" choice kicks in. That massive ten-pound pack of chicken breast at dirt cheap price ... we really have no idea of its origins or vintage. Wait ... we do have a rough idea. It was raised in a massive chicken farm owned by a corporate monopoly in methods and circumstances that will make you puke. Chicken (or cattle) that are cooped up in the dark, medicated, and force-fed continuously so that they attain maximum weight in the minimum time with minimum movement and metabolism. That's how corporates maximize profit. In India, you still have to the option of seeking out the healthier free-range or home-grown chicken, fresh locally grown- or sourced vegetables and fruits. You could be saying goodbye to all that (or at least end up paying much much more) with the FDI fiesta.
On a recent trip to the great American outback, your correspondent saw visual evidence of what this corporatization and industrialization of food production — widely seen as inevitable once the retail FDI gates are open — can do to the landscape and population. Thousands upon thousands of acres of farmland, typically owned or leased by corporates or large farming interests, grew bounteous harvests of corn (even in a drought year). This was not the corn, the "bhutta" from the push cart vendor that you eat with relish. It is mostly genetically modified, tasteless, industrial-grade rubbish that is aimed at maximizing yield. When it is not used as animal feed, it is turned into corn syrup which is used sweeten almost everything you see in the supermarket, including that sugary soft drinks you guzzle.
The result is all too visible in much of the US, nowhere more than the heartland of the country, where people come in large, economy size, with consequent health issues (obesity linked diabetes and heart disease). Much of this comes from eating cheap, low-quality, industrial grade food — from mass-produced breads and meat. There are few places in the world is where food available as cheaply (relative to income) as America. Till a couple of decades ago, Americans spent up to 15 per cent of their income on food; it is now below ten per cent and still dropping. It is now an accepted fact that the poorer the state in America, the more obese people are, because they are eating cheap, mass-produced food of the kind offered by fast-food chains. That dreadful burger and pizza and cola that you are wolfing down from the retail assembly line ... it's the cheapest and the worst kind of food you could be eating.
So here's the equation. If you allow the kind of retail revolution that has overtaken America, you could end up consuming cheap, low grade, mass-produced, industrial quality produce. Of course, it is easy to sniff down at all this from the high vantage point of those who have money in the pocket and the luxury of choice. But what about those with limited means who cannot afford to spend as much on fresh produce as corporatization of the food chain takes hold? So should be just reject the American/western way and stick to our current way, as many of those opposed to the Wal-Mart way are recommending? Then what happens to the farmers who seek better market access and greater returns, who want to eliminate waste and spoilage. Isn't FDI retail lucrative for him — at least to begin with, before predatory practices set in. Which way should we go? Will we, to paraphrase John Kerry, end up being "for it, before we turn against it?"
The answer, without it sounding like a cop-out, is to embrace the middle way. We need all the systems and logistics that FDI retail will bring, but we need to tweak it to make sure we don't go the American way. In some ways we should be reassured by what has happened already: the arrival of American retail food chains such as KFC, McDonalds, and Pizza Hut, did not destroy Indian eateries or Indian eating habits. We took the best practices from them, and today many Indian food outlets have the same look and feel of their western counterparts while continuing to serve the Indian palate. So the arrival of Wal-Mart may just herald the birth of the Agarwal-Mart.
Mike Maloney in Horrible Car Crash with Tesla | GoldSilver.com

Below is an awesome piece of writing by Mike Maloney about his horrible crash experience and comparing it with the impending economic crash underway....
A Sunday Drive In My Tesla.
This story is written in 4 parts:
Part 1. The Car Crash
Part 2. The Economic Crash
Part 3. The Cars
Part 4. Freedom and the Pursuit of Excellence
LINK:
Mike Maloney in Horrible Car Crash with Tesla | GoldSilver.com







